Archive of ‘Autism’ category
 As the spring semester is ending, let’s take a look at what we have discussed. First, we delved into the question of how autism spectrum disorder is diagnosed and what are some of the early signs of autism. A monitoring and screening tool was provided as a resource for parents as well.
As the spring semester is ending, let’s take a look at what we have discussed. First, we delved into the question of how autism spectrum disorder is diagnosed and what are some of the early signs of autism. A monitoring and screening tool was provided as a resource for parents as well.
It might be a tough question when deciding whether treatment is necessary for your child once they are diagnosed. Here are a couple of helpful suggestions to guide your decision-making process. There are many treatment options out there. It could be overwhelming sometimes, we presented applied behavior analysis and other treatment options that are listed by the CDC.
Then, we discussed one of the strategies called planned ignoring. even though it could be an effective intervention, it has to be combined with a reinforcement-based intervention. We also discussed situations in which planned ignoring should not be used. Not only we talked about consequence-based intervention but also, we suggested many antecedent-based strategies to help caregivers be more proactive. For example, using specific instructions, offering choices, and using visual schedules.
Behavior issues are not the only things that parents encounter. Many children have sleep issues. We introduced the bedtime pass and bedtime routines to facilitate better sleep habits for both children and adults.
Remember to visit and like our Facebook page for the latest update on ABA Husky Clinic and future blog posts.
 Sleep issues are common with pre-school and school-age kids. For parents, those issues could sometimes seem extremely difficult in terms of coming up with solutions. One strategy called bedtime pass could be a simple and effective way to address children having a hard time staying in their bedroom at night. Also, it has been shown to be effective for children who are diagnosed with autism.
Sleep issues are common with pre-school and school-age kids. For parents, those issues could sometimes seem extremely difficult in terms of coming up with solutions. One strategy called bedtime pass could be a simple and effective way to address children having a hard time staying in their bedroom at night. Also, it has been shown to be effective for children who are diagnosed with autism.
The bedtime pass is just like how it sounds. A 5×7 card is given to the child and the child can use the pass to get out of bed for any reason. It can be used to get a hug from the parents, grab something to drink, a bedroom visit. If the child is again out of the room once they have used the pass, the parent will neutrally guide the child back to their room. For most children, they will save the bedtime pass for later and then falling asleep. However, if your child is having a cold or discomfort that requires frequent visits throughout the night, the strategy should be postponed.
Let’s take a look at this strategy step by step:
- Provide a bedtime pass (a special card) and the card can be used by the child for many reasons (e.g., get a drink, a visit from parents, a hug from parents).
- Send your child to bed and make sure the bedtime pass is near the child (e.g., next to the pillow, in their hands).
- The card will be taken once the child used the bedtime pass that night.
- If children get out of the room after using the pass, parents will neutrally guide their children back to the bedroom.
Many times, during the first couple of nights, children will try to visit a couple more times to see if you are serious about the rules. After a few nights, they will hold on to the pass and make sure to use it when necessary.
We can also address sleeping problems on the front end, there are many bedtime routines shown to be effective in helping children stay in bed and sleep through the night. We will discuss those strategies next week. You can find other strategies on our Facebook page.
 So far, we have discussed many behavioral-based strategies that you can use at home and in other settings. For example, behavior-specific praise, shaping, and token economy. These strategies are helpful when you are with your child. However, what if your child is at school and the teacher reports that the child displays unwanted behavior such as disrupting in class, problems with transitions from one task to another? What can you do when you are not around? Teachers are usually extremely busy and have many children in one class to monitor and many lessons to plan. Thus, it is recommended not to rely on the teachers solely. Home-based reinforcement program (HBRP) could be beneficial.
So far, we have discussed many behavioral-based strategies that you can use at home and in other settings. For example, behavior-specific praise, shaping, and token economy. These strategies are helpful when you are with your child. However, what if your child is at school and the teacher reports that the child displays unwanted behavior such as disrupting in class, problems with transitions from one task to another? What can you do when you are not around? Teachers are usually extremely busy and have many children in one class to monitor and many lessons to plan. Thus, it is recommended not to rely on the teachers solely. Home-based reinforcement program (HBRP) could be beneficial.
HBRP is a method for effective behavior change in which your child’s behavior in school is reported to his or her parents who then reward the behavior. Here are the steps for an HBRP:
Be specific with the behavior: What is the behavior that the teacher and you are concern about in school? When defining the behavior make sure to be specific and both you and the teacher have the same definition in terms of what the behavior might look like.
Creating a system: There should be a system set up for the teacher to use when measuring your child’s behavior. Such as a Likert scale of 0 to 2. 0 means there is no change and unwanted behavior is still there and 2 means there is a drastic change in behavior and great improvement is observed by the teacher. At the end of the day, an index card with a point will be handed to you indicating how many points your child earned on that day.
Reward program or token economy: In a separate blog post we discussed the token economy. Similarly, your child earns the points based on the points that she received on that day in exchange for the predetermined rewards. Also, make sure there are various small and big rewards so your child can get smaller rewards immediately or save up tokens for bigger rewards.
To ensure that HBRP will be successful in changing unwanted behavior.
- Working with the teacher to focus on one behavior at a time.
- Your reactions to your child’s score are important to the success of the program.
- Make sure to celebrate small improvement, one of the pitfalls for the program is demanding perfection.
- When score is
- 0 – your response should be calm and do not complain or ask what happened because it might hinder the willingness of the child to participate in the program. For example, you can say “You did not get any points today but you can try again tomorrow.”
- 1 – Praise the slight improvement.
- 2 – Praise the perfect score enthusiastically.
HBRP is a useful strategy to address behavior issues in school and other settings. Most teachers are more than willing to participate as it does not demand a lot of effort and also helps change unwanted behavior.
For next week, we will discuss a behavioral strategy used for sleep problems with children called “bedtime pass”.
 Strategies such as planned ignoring and behavior-specific praise are consequence-based interventions. In other words, those strategies come after the behavior has happened. What if we can address the behavior on the front end? This is when Antecedent interventions come into play. Antecedent interventions are designed to change the environment or setting events before a particular behavior occurs to increase the likelihood of positive behavior. Board-certified behavior analysts (BCBAs) often manipulate antecedents to set up opportunities to prompt more positive behavior.
Strategies such as planned ignoring and behavior-specific praise are consequence-based interventions. In other words, those strategies come after the behavior has happened. What if we can address the behavior on the front end? This is when Antecedent interventions come into play. Antecedent interventions are designed to change the environment or setting events before a particular behavior occurs to increase the likelihood of positive behavior. Board-certified behavior analysts (BCBAs) often manipulate antecedents to set up opportunities to prompt more positive behavior.
There are many common types of antecedent strategies:
Using clear and specific instructions: It is important to keep in mind that when you ask your child to do something, be as specific as you can. For example, instead of saying “Go clean up your room.”, “Pick up 3 pieces of clothing on your bedroom floor.” Having clear and specific instructions is not only easier for your child to comply but also your child knows what is being expected. Of course, you do not need to always be so specific with your instructions, but it is helpful when you start developing positive behavior.
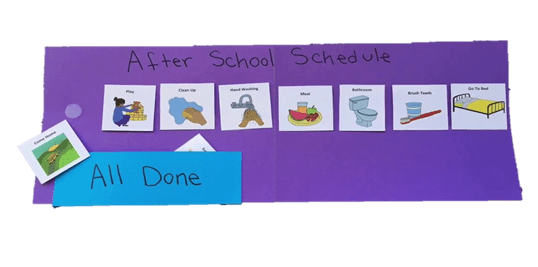
Visuals: Research has shown that individuals who are diagnosed with autism spectrum disorder tend to process visual cues better than auditory ones. Using visual schedules to present clear expectations. They are similar to planners we use for school or work but instead of listing all the tasks for the day.
Offer choices: Giving choices is a powerful tool to increase compliance. Using clear and specific instructions might be enough for your child. However, if you have any problems with compliance, by adding choice, you will increase the impact. For example, you could say to your child “Please put on your green gloves or brown gloves, we are going outside.” By offering a choice, it will greatly increase the chance that your child puts something on right away.
The three antecedent strategies mentioned above are helpful tools to increase compliance and decrease unwanted behavior. It is more effective if you combine them with reinforcement strategies (e.g., behavior-specific praise, token economy).
Next week, we will discuss an effective tool: Home-based reinforcement program (HBRP) to manage your child’s behavior in school settings.
 Last week, we introduced planned ignoring to guide your child’s behavior. The idea of planned ignoring is that you deliberately withhold your attention when unwanted behaviors occur. Attention is a powerful reinforcer that you might not realize. Sometimes, even reprimands or negative attention could serve as a reinforcer for children. The questions are how to make planned ignoring more effective and if it is suitable for you and your child.
Last week, we introduced planned ignoring to guide your child’s behavior. The idea of planned ignoring is that you deliberately withhold your attention when unwanted behaviors occur. Attention is a powerful reinforcer that you might not realize. Sometimes, even reprimands or negative attention could serve as a reinforcer for children. The questions are how to make planned ignoring more effective and if it is suitable for you and your child.
One of the most difficult aspects is ignoring. As sometimes, it is extremely difficult to not give in from time to time. Here are some tips when using planned ignoring:
- Plan ways to distract yourself: You should always be proactive and find things or ways to distract yourself from attending to the behavior. You could put on some music, breathe deeply, or think of something irrelevant such as planning your shopping list.
- Start withholding your attention when the behavior starts and provide attention right away when the behavior stops.
- Always give your child positive attention and praise for positive behavior or the alternative behavior. In other words, the behavior you want to see instead.
As not every strategy is suitable for every situation. Here are questions that help you to answer whether planned ignoring is right for you and your child:
Can I ignore the behavior if it gets worse?
We talked about extinction burst in which you would see an expected increase in unwanted behavior. For example, if the unwanted behavior is tapping the table and once you start withholding your attention, they start slamming the table. If you feel that you cannot deal with and simply ignore the behavior, it is better to stick to reinforcement-based strategies.
Should you ignore the behavior?
Some behavior cannot be ignored for obvious reasons. You cannot ignore behaviors that might harm themselves, others.
Is the behavior also reinforced by other’s attention?
The unwanted behaviors could also be maintained by other’s attention. For example, another caregiver, siblings, friends. Therefore, it is difficult to see the desired results when only you are withholding attention for the behavior.
Planned ignoring is not suitable for everyone and every situation. Therefore, you should ask your board-certified behavior analysts (BCBAs) for suggestions.
We will switch gears next week and discuss antecedent strategies that could address unwanted behaviors before they happen.
 In a previous blog, we discuss the strategy of catching children’s good behavior. Another strategy that could be used is called planned ignoring. Planned ignoring is when you deliberately withholding attention when the child is engaging in behavior that you do not want to see, and the behavior would be less likely to happen in the future. It might sound simple enough to implement. However, there are a couple of things that need to be noted to see effective results.
In a previous blog, we discuss the strategy of catching children’s good behavior. Another strategy that could be used is called planned ignoring. Planned ignoring is when you deliberately withholding attention when the child is engaging in behavior that you do not want to see, and the behavior would be less likely to happen in the future. It might sound simple enough to implement. However, there are a couple of things that need to be noted to see effective results.
- Consistency is key
When withholding attention for unwanted behaviors, keep it consistent. In order words, you should be clear with your expectation and the child will understand that the particular behavior will not result in the consequence (reward) they had in the past. For example, your child might yell loudly, as a result, she gets your attention. Now, you would look away or walk out of the room.
- Reinforce other behavior
Planned ignoring should NOT be used alone. Reinforcement-based procedures should always be used in conjunction with planned ignoring. Providing attention when the child engages in behavior that you want to see more of. You need to make sure that the child knows what to do instead. For example. When your child asks for your attention by tapping you in the back, make sure to provide your undivided attention and deliver behavior-specific praise.
- Extinction burst
Extinction bursts are sudden and expected increases in unwanted behavior. Therefore, when you first look away or walk out of the room when your child yells for attention, you might hear your child yells louder as a result. We encounter extinction bursts more often than you think. Think of the time you push an elevator button to close the door. As most of the time, the door does not close immediately. What do you do usually? You push a couple more times or pushing it harder. Therefore, the procedure is working when you see an expected increase in behavior.
Planned ignoring is a strategy that is not easy to implement as you can imagine it is extremely difficult to not give in from time to time. Extinction burst often is not easy to tolerate for most caregivers. Here are some takeaway points:
- NOT using planned ignoring alone: When a board-certified behavior analyst (BCBA) use planned ignoring, Reinforcement based strategies are always used. Attention or praise will be provided for positive behavior to teach the child what to do instead to get attention. For example, if your child is bouncing up and down during dinner time, you could leave them out of your conversation and not looking at them until they sit in the chair nicely. Then, you will immediately say “I love how you sit in your chair. Can you tell us more about your day at school today?”
- It gets worst so it is working: Remember the unwanted behavior tends to get worst for a short period before it gets better. When a BCBA implements planned ignoring, many parents are concerned because the behavior seems to get worst. Having extinction burst in mind will help you to follow through with the plan put in place by a BCBA.
Next week, let us examine some of the tips when using planned ignoring and if this tool is the best option for you and your child.
 When it comes to selecting the best treatment for your child, the CDC lists several treatment options for children diagnosed with ASD in four categories (e.g., behavior and communication approach, Medication, Dietary Approaches). Under behavior and communication approaches, applied behavior analysis (ABA) is one of the approaches mentioned. But why should you consider ABA out of other treatment options? You might ask. Several reasons make ABA stands out, among others:
When it comes to selecting the best treatment for your child, the CDC lists several treatment options for children diagnosed with ASD in four categories (e.g., behavior and communication approach, Medication, Dietary Approaches). Under behavior and communication approaches, applied behavior analysis (ABA) is one of the approaches mentioned. But why should you consider ABA out of other treatment options? You might ask. Several reasons make ABA stands out, among others:
- Applied behavior analysis focuses on evidence-based practices: ABA therapists use interventions that have been demonstrated to be effective in studies. As children received early intensive services, it can lead to meaningful changes in behavior and skills for children diagnosed with ASD.
- Various applied settings: ABA is flexible in terms of learning environments. The therapists always adjust to each family’s needs. There are home-based, school-based, and clinic-based services. Different from many services, ABA does not have to take place in an isolated therapy space. As generalization is one of the main goals. ABA therapists encourage various spaces.
- Planning for generalization: As skills child learned should not only be performed in one particular space. For example, we would like the child to ask for attention appropriately not only at home but in school as well. Therefore, ABA helps to generalize the skills by simulate natural environments to make the generalization of skills easier.
- Inclusion of caregivers: Involvement from caregivers is one of the essential aspects that promote successful treatments. Caregivers are often encouraged to participate in the therapeutic processes in terms of learning effective skills in dealing with daily concerns and deciding treatment goals. This involvement often reduces stress at home as traditional parenting techniques are seldomly effective for children diagnosed with ASD.
When deciding treatment options that would be effective and most suitable for your child, it is important to be a critical consumer and ask questions. There are a few questions that help identify viable treatment options:
- What is the treatment that the therapist is going to provide?
- How long has the therapist been providing the particular treatment?
- Has the particular treatment been studied, and has scientific evidence in its favor?
- What are the treatment options besides the one the therapist provides?
Don’t forget Husky ABA Clinic is a wonderful resource for you if you have other questions.
 In the previous blog, we discussed what the diagnostic process could look like for a child diagnosed with autism spectrum disorder (ASD). As the name entails, ASD is a spectrum in which the child could have severe to relatively mild symptoms. Treatment services are necessary when the behavior is rather severe but what if you are having a difficult time deciding whether seeking professional help is right for your child?
In the previous blog, we discussed what the diagnostic process could look like for a child diagnosed with autism spectrum disorder (ASD). As the name entails, ASD is a spectrum in which the child could have severe to relatively mild symptoms. Treatment services are necessary when the behavior is rather severe but what if you are having a difficult time deciding whether seeking professional help is right for your child?
Here are some helpful suggestions to guide your decision-making process:
Dangerous behaviors: Your child is engaging in behavior that is harmful to themselves or others to the extent that is interfering with daily routines and activities.
Lack of communicative skills: Your child does not respond when you call his or her name and lack eye contact.
Repetitive behaviors: Does your child engages in repetitive behavior with toys or objects for hours?
Showing signs of delay development:
- Doesn’t respond with a smile or happy expression by 6 months
- Doesn’t mimic sounds or facial expressions by 9 months
- Doesn’t babble or coo by 12 months
- Doesn’t gesture — such as point or wave — by 14 months
- Doesn’t say single words by 16 months
- Doesn’t play “make-believe” or pretend by 18 months
- Doesn’t say two-word phrases by 24 months
- Loses language skills or social skills at any age
Keep in mind infants and toddlers tend to develop at their own pace and do not follow the timelines found in most parenting books exactly. However, Signs of ASD often appear early in development when there are obvious delays in language skills and social interactions. You should pay close attention and consider seeking professional help if your child has delays in those aforementioned skills.
Next time, we would explore some of the effective treatment options and resources in terms of seeking treatments. Follow us on Facebook to explore more resources.
 Autism spectrum disorder (ASD) is a developmental disorder that usually impacts an individual in terms of social interaction and communication. Some children may show signs of ASD as early as infancy. Typically, the child will show a lack of eye contact, reduced response to their name, or restricted and repetitive behaviors. However, no two children diagnosed with ASD are alike; therefore, how doctors diagnose ASD may vary. Due to the variabilities of severity, there is not a specific medical test to determine the disorder. Usually, pediatricians are the first professionals involved in the autism diagnosis process. As children get an assessment during their well-child visits that occur at 18-and 24-months. Your child’s doctor will be looking for things such as: whether your baby started babbling and cooing by 12 months, if they were mimicking sounds and facial expressions by 9 months, or if your baby smiled by 6 months.
Autism spectrum disorder (ASD) is a developmental disorder that usually impacts an individual in terms of social interaction and communication. Some children may show signs of ASD as early as infancy. Typically, the child will show a lack of eye contact, reduced response to their name, or restricted and repetitive behaviors. However, no two children diagnosed with ASD are alike; therefore, how doctors diagnose ASD may vary. Due to the variabilities of severity, there is not a specific medical test to determine the disorder. Usually, pediatricians are the first professionals involved in the autism diagnosis process. As children get an assessment during their well-child visits that occur at 18-and 24-months. Your child’s doctor will be looking for things such as: whether your baby started babbling and cooing by 12 months, if they were mimicking sounds and facial expressions by 9 months, or if your baby smiled by 6 months.
The following are other questions that the doctor might ask you as the caretaker:
- Does your child have trouble making eye contact?
- Do they have any unusual or repetitive behaviors?
- Are they sensitive to light, noise, or temperature?
- Do they respond when others seek their attention?
More tests would be required for further examination if your child’s doctor suspects that your child might be at risk of ASD. Specialists such as child psychologists, speech-language pathologists, and occupational therapists will provide more comprehensive tests. These tests consist of checking your child’s cognitive level, language abilities, and fine motor skills such as pointing, shaking objects, or drinking from a sippy cup.
There are two critical aspects that would make the specialist more inclined to diagnose your child with ASD:
Restricted and repetitive patterns of behavior: Commonly, children diagnosed with ASD might repeat phrases, rock their bodies, fixate on one subject, or are extremely sensitive to changes in routines.
Challenges with communication and social interaction: Children diagnosed with ASD have a hard time making connections or predicting the reactions of other people. Also, they could be missing the milestones of speaking compared to other children.
As parents, if you are concerned, make sure to contact your child’s doctor. This developmental monitoring and screening tool could be helpful as general milestones guidelines for your child.
Our Husky ABA Clinic is also a great resource to provide directions if you have more questions. Once your child is diagnosed, how will you decide if treatment is necessary for your child? Next week, we will delve into some of the determining factors when seeking treatment options.





